Translating Strategies for Promoting Engagement in Mobile
Health: A Proof-of-Concept Micro-Randomized Trial
Inbal Nahum-Shani,
Institute for Social Research, University of Michigan
Mashfiqui Rabbi,
Department of Statistics, Harvard University
Jamie Yap,
Institute for Social Research, University of Michigan
Meredith L. Philyaw-Kotov,
Department of Psychiatry and Addiction Center, University of Michigan
Predrag Klasnja,
School of Information, University of Michigan
Erin E. Bonar,
Department of Psychiatry and Addiction Center, Injury Prevention Center, University of Michigan
Rebecca M. Cunningham,
Department of Emergency Medicine, Injury Prevention Center, School of Public Health, University
of Michigan
Susan A. Murphy,
Departments of Statistics & Computer Science, Harvard University
Maureen A. Walton
Department of Psychiatry and Addiction Center, Injury Prevention Center, University of Michigan
Abstract
Objective: Mobile technologies allow for accessible and cost-effective health monitoring and
intervention delivery. Despite these advantages, mobile health (mHealth) engagement is often
insufficient. While monetary incentives may increase engagement, they can backfire, dampening
intrinsic motivations and undermining intervention scalability. Theories from psychology and
behavioral economics suggest useful non-monetary strategies for promoting engagement; however,
examinations of the applicability of these strategies to mHealth engagement are lacking. This
proof-of-concept study evaluates the translation of theoretically-grounded engagement strategies
into mHealth, by testing their potential utility in promoting daily self-reporting.
Methods: A micro-randomized trial (MRT) was conducted with adolescents and emerging adults
with past-month substance use. Participants were randomized multiple times daily to receive
theoretically-grounded strategies, namely reciprocity (the delivery of inspirational quote prior to
Contact Information: [email protected].
HHS Public Access
Author manuscript
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Published in final edited form as:
Health Psychol
. 2021 December ; 40(12): 974–987. doi:10.1037/hea0001101.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
self-reporting window) and non-monetary reinforcers (e.g., the delivery of meme/gif following
self-reporting completion) to improve proximal engagement in daily mHealth self-reporting.
Results: Daily self-reporting rates (62.3%; n=68) were slightly lower than prior literature, albeit
with much lower financial incentives. The utility of specific strategies was found to depend
on contextual factors pertaining to the individual’s receptivity and risk for disengagement. For
example, the effect of reciprocity significantly varied depending on whether this strategy was
employed (vs. not employed) during the weekend. The non-monetary reinforcement strategy
resulted in different outcomes when operationalized in various ways.
Conclusions: While the results support the translation of the reciprocity strategy into this
mHealth setting, the translation of non-monetary reinforcement requires further consideration
prior to inclusion in a full scale MRT.
Keywords
Engagement; Mobile Health (mHealth); Micro-Randomized Trial (MRT); Reciprocity;
Reinforcement; [ClinicalTrials.gov: NCT03255317]
Introduction
Mobile technologies allow for accessible and cost-effective health monitoring and
intervention delivery. Their widespread use, acceptability and convenience can help reduce
barriers to health care access and utilization (Amico, 2015), and enhance scalability across
geographic locations (Haberer et al., 2017). Mobile devices are also capable of giving round-
theclock, real-time reminders, intervention prompts and feedback. Smartphones and tablet
computers are able to host applications (apps) with a multitude of capabilities (e.g., social
networking, gaming) (Pellowski & Kalichman, 2012). A recent meta-analysis of mobile
health (mHealth) intervention studies among youth concluded that mHealth is an effective
modality for promoting health behavior change (Fedele et al., 2017).
Despite these advantages, engagement in mHealth tools is often too limited to support
behavior change (Michie et al., 2017). Engagement is defined as a state of energy investment
directed toward a focal task or stimulus (Shaw et al., 2019), which involves cognitive (e.g.,
attention), affective (e.g., positive feelings) and behavioral (e.g., participation) aspects (King
et al., 2014). In mHealth interventions, the focus has been mainly on behavioral aspects of
engagement (e.g., frequency, duration, or depth of usage) (Perski et al., 2016). Empirical
evidence indicates that adequate usage of such tools is rare (Dobson et al., 2017; Saberi &
Johnson, 2015), and least likely among those with poor self-reported health (Robbins et al.,
2017). Thus, promoting adequate engagement with mHealth tools is of critical importance
(Roberts et al., 2017).
While monetary incentives can increase mHealth engagement, relying on monetary
incentives alone may backfire, dampening intrinsic motivations (Strang et al., 2016), leading
to unintended consequences (e.g., inappropriate use of incentives increasing risk behavior;
Kohler & Thornton, 2012) and undermining scalability. Hence, a richer toolset of incentives
is clearly needed (Linnemayr & Thomas, 2016). Research in psychology, human computer
interaction (HCI), and marketing highlights alternative engagement strategies, including
Nahum-Shani et al.
Page 2
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
social influence tactics (Cialdini & Goldstein, 2004), behavioral economics principles (Haff
et al., 2015), and gamification (e.g.,Taylor et al., 2019). However, limited research attention
has been given to optimizing theory-based engagement strategies in mHealth settings, where
the goal is to engage individuals in their natural environment despite multiple demands
competing for their time, effort and attention.
To address this gap, the current study was designed to build a research foundation for
promoting engagement in mHealth tools. The mobile app used in the current study
(Substance Abuse Research Assistant [SARA]) was motivated by evidence indicating that
substance use among adolescents and emerging adults (A/EAs) is associated with the
leading causes of morbidity and mortality (Hingson et al., 2017; Patrick et al., 2017).
Increasing the frequency of self-reporting for substance use and related factors among youth
is important from research (e.g., understand behavior change processes) and intervention
perspectives (e.g., capitalize on the therapeutic gains of self-monitoring) (French & Sutton,
2010; Swendeman et al., 2015). Given research showing suboptimal engagement with self-
reporting of substance use (Roberts et al., 2017), this proof-of-concept study examined
the potential utility of theoretically-grounded strategies to promote engagement in daily
mHealth self-reporting among substance-using A/EAs.
We begin by presenting a logic model (Figure 1) to help organize the engagement strategies
integrated in SARA and then discuss scientific questions that motivate the investigation of
two specific strategies. The first strategy--
reciprocity
-- refers to the provision of a small
unsolicited gift to capitalize on the innate psychological tendency to return favors and other
acts of kindness (Cialdini, 2001; Perugini et al., 2003). The second strategy --
non-monetary
reinforcement
-- refers to providing conditional rewards that are hedonic in nature, based on
entertainment and exploration (Coker et al., 2014). We then describe a micro-randomized
trial (MRT) conducted with 68 A/EAs screening positive for binge drinking or marijuana
use, who were instructed to self-report substance use and related factors via the SARA
app for 30 days, and were micro-randomized daily to engagement strategies. We discuss
results pertaining to the potential utility of reciprocity and non-monetary reinforcement in
promoting mHealth self-reporting. The research questions and hypotheses motivating the
MRT were specified a priori (Rabbi et al., 2017). Guided by the NIH Stage Model (Onken
et al., 2014) and the Multiphase Optimization Strategy (MOST; Collins, 2018), we discuss
implications for future research on promoting mHealth engagement.
A Logic Model for Integrating Engagement Strategies
Extant literature on engagement in learning activities (Butler & Nisan, 1986; Efklides,
2011), behavioral interventions (De Young, 2000; King et al., 2014; Lizardi & Stanley,
2010), and technology-based interventions (Cavanagh, 2010; Perski et al., 2016) highlight
three interrelated constructs which determine the likelihood of engagement in an activity.
Need recognition
1
reflects an individual’s awareness of a discrepancy between his/her
present state and a preferred future state (Allen et al., 2014; Fox & Miner, 1999);
1
Need recognition relates to the concept of self-discrepancy, which reflects a conflict or inconsistency between different aspects of
the self (Higgins et al., 1986). A number of empirically-supported psycho-therapeutic approaches address such conflict, including
Motivational Interviewing (Miller & Rollnick, 1991) and Acceptance and Commitment Therapy; see discussion in (Kelly et al., 2015).
Nahum-Shani et al. Page 3
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
ability, reflects the extent to which an individual has the knowledge, experience, skills
and capacity to engage in the activity (Kleinginna & Kleinginna, 1981); and motivation,
reflects the extent to which an individual is willing to engage (Rivis et al., 2011). The
engagement strategies in SARA are consistent with the Need, Ability & Motivation (NAM)
logic model.
2
To increase need recognition for self-reporting, SARA uses self-regulatory
techniques (Carver & Scheier, 1982), including: setting clear goals for self-reporting,
monitoring self-reporting via the app, and providing feedback. To enhance the participant’s
cognitive ability to engage in self-reporting, reminder notifications are provided to address
forgetfulness. Finally, to enhance motivation to self-monitor, engagement is reinforced via
a point system and a virtual aquarium, which starts empty, but displays more fish and
treasures as the participant engages in daily self-reporting (see Rabbi et al., 2018). A more
detailed conceptual diagram describing the different engagement strategies in SARA is
provided in Rabbi et al (2017; Figure 3). Below, we provide the scientific rationale for
testing two theoretically-grounded strategies for increasing motivation to engage: reciprocity
and non-monetary reinforcement (Rabbi et al., 2017).
Reciprocity
The meta-norms of reciprocity are a suite of social rules maintaining that people should
return favors and other acts of kindness (Gouldner, 1960). Performing a small, often
unsolicited, favor can trigger these norms, increasing the likelihood that the recipient will
later agree to a subsequent request from the favor-giver. Marketing strategies such as free
gifts are common experiences for consumers, who may feel obligated to buy the product
(Burger et al., 2009). Individuals may return favors out of concerns for what others may
think of them (e.g., that they will be viewed ungrateful or as freeloaders; Cialdini, 2001)
and/or because they internalize the reciprocity norms as a personal standard (Perugini et
al., 2003). Hence, people feel good about themselves when they return favors, and chastise
themselves when they fail to reciprocate.
Empirical evidence indicates that receiving help, gifts, favors, or concessions motivates
people to reciprocate (Cialdini, 2001; Cialdini & Goldstein, 2004), including in human-
computer interactions (Fogg, 2002; Fogg & Nass, 1997), human-robot interactions (Lee &
Liang, 2016), and technology-facilitated social interactions (Parsons et al., 2019). However,
no attempt has been made to investigate whether the norms of reciprocity can be capitalized
on to increase mHealth engagement. In SARA, the provision of a small unsolicited reward
was operationalized by offering an inspirational quote two hours prior to the start of the
self-reporting window. Inspirational quotes were selected because (a) they are non-monetary
in nature; and (b) preliminary formative research indicated that this type of content is valued
by the target population (Rabbi et al., 2018). We posed the preliminary hypothesis:
H1
3
: Offering (compared to not offering) a small, unsolicited reward in the form of an
inspirational quote increases the likelihood of self-reporting on the current day.
2
Related models exist, such as the COM-B system (Michie et al., 2011) for understanding behavior.
3
Hypotheses 1, 2 and 3 were pre-specified in Open Science (Rabbi et al., 2017). H1 and H2 were specified as primary hypotheses, and
H3 was specified as one of two secondary hypotheses.
Nahum-Shani et al. Page 4
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Non-Monetary Reinforcement
Grounded in behavioral theory (i.e., operant conditioning), reinforcement — defined as “the
process in which the occurrence of a behavior is followed by a consequence that results
in an increase in the future probability of the behavior” (Miltenberger, 2011, p. 513) —
is a wellestablished method for enhancing compliance (Shelton & Levy, 1981). A positive
reinforcer is a stimulus that increases future behavior. In psychotherapy and coaching, verbal
praise is a common reinforcer (Hancock, 2000), which does not have to involve actual
social presence (i.e., a therapist) to be effective; Fogg (2002) found that a single dialog
box praising the individual can enhance engagement. For a reinforcer to be effective, it
should occur immediately after the target behavior (Miltenberger, 2011), which is easily
accomplished in mHealth (Lent, 2017), and involve a greater magnitude for more complex
behaviors (McPherson et al., 2018).
We tested two forms of non-monetary reinforcers:
entertaining content
, operationalized
as a meme or an animated gif (funny or inspirational), and
personalized information
4
,
operationalized as visual data summaries. The first form is based on literature in positive
psychology (e.g., Fredrickson, 2004) and learning (e.g., Pekrun, 2006) which posits
that positive emotions facilitate increased effort, widening attention, promoting intrinsic
motivation, and facilitating the use of flexible cognitive strategies (e.g., planning). Although
offering mHealth content that promotes positive emotions could reinforce activities that
require low effort (e.g., daily self-reporting), this has not been empirically established.
The second form is based on research in the area of cognitive and social psychology
(Brown & Dutton, 1995; Hull et al., 1988) which indicates that people strive to manage
uncertainty by seeking and attending to information about themselves (Derricks & Earl,
2019; Leonardelli & Lakin, 2010; Van den Bos, 2009). Although people are interested in
receiving personalized data (Rabbi et al., 2018; Singh et al., 2016), it is unclear whether such
information reinforces mHealth self-reporting. Thus, we pose the preliminary hypotheses:
Offering (compared to not offering) a non-monetary reinforcer in the form of entertaining
content (H2
3
); or in the form of personalized information (H3
3
) immediately following
self-reporting, increases the likelihood of self-reporting on the next day.
Indicators of Vulnerability and Receptivity as Moderators
Organizing frameworks for constructing mHealth interventions emphasize the importance
of delivering intervention prompts (e.g., cues to induce desired responses) (Raes et al.,
2012) not only when the individual is vulnerable, but also in a manner that minimizes
disruptions, that is, only when the individual is receptive.
Vulnerability
refers to the
person’s transient tendency to experience negative outcomes (hence indicating need for an
intervention), and
receptivity
refers to the person’s transient tendency to receive, process,
and use intervention prompts (Nahum-Shani et al., 2015). In the context of enhancing
mHealth engagement, vulnerability can be conceptualized as conditions that represent
increased risk for disengagement, indicating need for an engagement strategy. Receptivity
can be conceptualized as conditions in which a particular strategy is likely to increase
4
Personalized information is labeled ‘life insights’ in previous descriptions of this study’s protocol.
Nahum-Shani et al. Page 5
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

engagement. Limited research attention has been given to identifying states of vulnerability
to disengagement and receptivity to engagement strategies (Morrison et al., 2017).
Here, we explored four moderators (which were specified as covariates a priori: Rabbi
et al., 2017) to identify the conditions in which individuals might be more vulnerable to
disengagement, and more receptive to engagement strategies. With respect to vulnerability,
two moderators were considered: prior self-reporting and app usage for other reasons (i.e.,
outside of self-reporting). Empirical evidence suggests that low engagement with mHealth
technology increases the risk for future disengagement (Simblett et al., 2018), indicating the
need for an engagement strategy (Karekla et al., 2019). Thus, mHealth prompts containing
engagement strategies may be more effective if the individual did not self-report in the
previous day or did not use the mobile app for other reasons. Regarding receptivity,
two moderators were considered: day of the week (weekdays vs. weekend), and whether
support was previously provided by study staff. Prior work suggest that individuals are
more receptive to mobile prompts during the weekends (Bidargaddi et al., 2018) and human
contact increases accountability and motivation (Karekla et al., 2019; Mohr et al., 2011),
hence facilitating receptivity to prompts. Thus, prompts containing engagement strategies
may be more effective during the weekend and if human support (e.g., reminders) was
provided (here, by study staff).
H4: The effects of the engagement strategies (reciprocity and non-monetary reinforcement)
on self-reporting are amplified under conditions that represent vulnerability to
disengagement (i.e., no prior self-reporting or app usage for other reasons) and receptivity to
engagement strategies (i.e., during the weekend and after receiving support from study staff).
Method
Study Design
This proof-of-concept study employed a micro-randomized trial (MRT) – an experimental
design for optimizing mHealth interventions (Liao et al., 2016). This study was intended
as an early check on translating theoretically-based engagement strategies to a particular
mHealth setting. These activities are consistent with
Stage I
of the NIH Stage Model (Onken
et al., 2014), which focuses on intervention creation, refinement and preliminary testing,
as well as with the
preparation
phase of the Multiphase Optimization Strategy (MOST)
(Collins, 2018), which focuses on laying the groundwork for optimizing a multi-component
intervention. Here, optimization refers to gathering information to decide what set of
components to include and how in order to comprise an effective and practical mHealth
intervention, prior to evaluating its effectiveness relative to control (Collins, 2018). Guided
by these frameworks, the MRT was employed to prepare for a fully powered optimization
MRT, by testing the potential utility of two theoretically-grounded strategies (reciprocity and
non-monetary reinforcers) in promoting mHealth engagement.
Participants
Participants were recruited and screened in the University of Michigan Hospital Pediatric
and Adult Emergency Departments. The study was approved by the Institutional Review
Nahum-Shani et al.
Page 6
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Board of the University of Michigan (HUM00121553) and is registered at ClinicalTrials.gov
(NCT03255317). Individuals were eligible for screening if they were 14–24 years old,
understood English, were medically stable, able to provide informed consent or assent, and
were accompanied by a parent or guardian (if 17 years old or younger). Screened individuals
were eligible for the MRT if they had access to a mobile phone (Android or an iPhone)
at enrollment and if they screened positive for past-month binge drinking (≥4 drinks for
females and ≥5 drinks for males) and/or past-month marijuana use (without a medical
marijuana card).
Procedures
Recruitment: Incoming admissions were reviewed (August 2017 - February 2018) to
identify patients aged 14 to 24 who met inclusion criteria to approach (Figure 2).
Participants (n=271, 85.2%) completed consent/assent and a screening survey on a tablet
assessing demographics, past-month health behaviors (e.g., alcohol and marijuana use) and
cell phone capabilities (see details in Rabbi et al., 2018). Participants received a small gift
valued at US $1.00 (e.g., headphones, water bottle). Those who met substance use and
cell phone inclusion criteria (n=111; 40.9%) were eligible for the MRT, and 74 (66.6%)
consented/assented, of which 68 were able to be included in the analyses (ages 17–24), and
59 (79.7%) completed a one-month follow-up. For this proof-of-concept study, recruitment
continued until project funds were spent.
Intake session: Participants enrolled in the MRT completed a baseline survey assessing
substance use and motivation to reduce alcohol and marijuana (see Rabbi et al., 2018),
provided their contact information, installed the SARA app, and received US $20.
Micro-randomizations: Participants started a 30-day MRT, where they were asked to use
the SARA app to complete one survey and two active tasks between 6pm and midnight
daily. The present analytical sample comprised the 68 (91.9%) participants who installed the
SARA app and completed at least one daily survey. To investigate the utility of reciprocity,
participants were randomized at 4pm each day with a fixed 0.5 probability to either a prompt
(via a push notification) containing an inspirational quote or no prompt. To investigate the
utility of non-monetary reinforcement, each day, if the participant completed the survey,
they were randomized with a fixed 0.5 probability to either a reinforcer in the form of
entertaining content or no reinforcer, and if the participant completed the active tasks
they were randomized with a fixed 0.5 probability to either a reinforcer in the form of
personalized information, or no reinforcer. Study staff who had contact with participants
were blinded to the random assignments.
One-month follow-up interview: Approximately one month after the intake visit,
participants completed a follow-up assessment (all by telephone except 1 in-person),
which included the baseline measures, a 30-day Timeline Follow Back calendar to capture
alcohol and marijuana consumption (Hoeppner et al., 2010), and questions to capture user
experience and acceptability of the SARA app (Stoyanov et al., 2015). Participants received
a US $30 electronic gift card of their choice (e.g., Amazon, Starbucks or Netflix).
Nahum-Shani et al.
Page 7
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Mobile-based self-reporting: The SARA app collects data via two active tasks
(Research Kit, 2018) and daily surveys. The spatial memory task displays a random
sequence of five seashells that light up in a 2-dimensional grid of nine seashells and
asks participants to repeat the sequence. The reaction time task includes two buttons that
participants are asked to tap alternately for 10 seconds. These tasks were selected given that
spatial memory and reaction time may vary depending on substance use-related intoxication.
The daily survey included 7 questions about factors associated with substance use, such
as stress level, loneliness, and amount of free time. On Sundays, the survey included 14
additional questions about substance use and motives in the past week (see Rabbi et al.,
2018 for details). Participants were asked to complete the daily survey and active tasks
between 6pm and midnight in order to provide (a) sufficient time for self-reporting; (b) an
opportunity for participants to reflect on most of the day while responding to the survey, and
(c) an opportunity to capture intoxication via active tasks since substance use among youth
typically occurs in the evening (Wray et al., 2014).
Contact by study staff: Contact by study staff was provided between 9pm – 10pm each
night based on non-completion using a pre-specified message template (see Rabbi et al.,
2018); thus, these reminders were not randomized. Specifically, a text message reminder
was sent following two days of non-completion of the daily survey or active tasks. If non-
completion continued for three additional days, a second text message was provided. After
7 consecutive days of non-completion, participants received a phone call from study staff.
Occasionally, study staff sent reminders via email or private social media messages based
on participants’ preference, or if they had an out-of-service cell phone number, or had been
nonresponsive to previous texts and phone calls. Text messaging and phone calls stopped if
participants neither responded nor self-reported for 3 weeks (n=6), or if a participant asked
to be removed from the study (n=1).
Minimal financial incentives: Participants earned US $1 for every 3 consecutive days of
daily self-reporting, and 50 cents for completing the longer Sunday survey. The rationale for
including minimal financial incentives along with a non-monetary intervention is provided
in Rabbi et al. (2018). For a 90% completion rate, most participants would earn US $12 or
less over the 30-day study (US $13 if completion rate is 100%). This is a fraction of what
substance use studies typically pay for daily self-reporting (e.g., US $2–5 per day) (Bonar et
al., 2018; Buu et al., 2017; Dworkin et al., 2017; Heron et al., 2019).
Randomized engagement strategies: The MRT investigated two engagement
strategies; both were developed in a prior user-centered design process (see Rabbi et al.,
2018).
Reciprocity:
At 4pm every day (two hours before the self-reporting window opened),
participants were randomized to either a prompt containing an inspirational quote or no
prompt. This timing was selected (a) to accommodate the typical daily routine of A/EAs
(e.g., they may be more likely to attend to a notification after school hours); and (b) to be
sufficiently close to the start of the self-reporting window (6pm). The inspirational quotes
(i.e., song lyrics and celebrity quotes) were selected by undergraduate research assistants to
make them age-appropriate.
Non-monetary reinforcement:
This strategy was operationalized
and tested in two ways. First, upon completion of the daily survey, participants were
Nahum-Shani et al.
Page 8
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
randomized to either a non-monetary reinforcer in the form of entertaining content or
no reinforcer. The reinforcer included a meme or an animated gif, intended to be either
funny or inspirational. This content was generated via Amazon’s Mechanical Turk, and
selected by undergraduate research assistants. Second, upon completion of the daily active
tasks, participants were randomized to either a non-monetary reinforcer in the form of
personalized information or no reinforcer. The reinforcer included a visual summary line
graph of past seven days of data (e.g., stress, tapping speed). Both reinforcers were
iteratively developed and preliminary tested prior to the MRT, with initial results indicating
that they were both well liked and perceived as rewarding by the target population (Rabbi et
al., 2020).
Measures
Feasibility: Building on prior work (Bonar et al., 2018; Stoyanov et al., 2015), feasibility
was measured by: (1) completion of daily surveys, weekly surveys and active tasks; (2)
amount of money earned during the 30-day MRT; and questions in the 1-month follow-
up, including (3) subjective engagement measured by ratings of “fun” and “interesting”
(Likert scale: 0=Not at all, 1=A Little, 2=Somewhat, 3=Moderately, 4=Very much so),
and the age-appropriateness of content (Likert scale: 0=Not at all to 2=Very much); (4)
acceptability of the inspirational quotes, memes/gifs, and personalized information (Likert
scales: 1=Strongly dislike to 5=Strongly like); (5) subjective burden, measured by ratings
of “easy to use” (Likert scale: 0=Not at all to 4=Very much so); frequency of technical
problems (range: 0=Never to 3=Regularly); and (6) satisfaction, measured by preference to
self-report using the app, phone or text message surveys, or either; and overall app rating
(scale: 1 to 5 stars in 0.5 star increments).
Proximal self-reporting (proximal outcome): To test the effect of reciprocity, the
proximal outcome is current day self-reporting—a binary indicator for whether (=1) or not
(=0) the survey or the active tasks were fully completed on the same day. To test the effect
of non-monetary reinforcement, the proximal outcome is next day self-monitoring-- a binary
indicator for whether (=1) or not (=0) the survey or active tasks were completed on the
following day.
Covariates/Moderators: Consistent with the Open Science registration (Rabbi et al.,
2017), the covariates are as follows.
Prior day self-reporting:
a binary indicator for whether
(=1) or not (=0) the survey and/or active tasks were completed in the prior day.
Prior app
usage for other reasons:
a binary indicator for whether (=1) or not (=0) the app was used for
activities unrelated to survey or active tasks completion prior to randomization (e.g., opening
the app to look at the virtual aquarium or unlock a fish). For the analyses of reciprocity, this
indicator was calculated based on the 72 hours
5
prior to micro-randomization to employing
(vs. not employing) the strategy. For the analyses of non-monetary reinforcement, this
indicator was calculated based on the 80 hours
5
prior to micro-randomization to employing
5
These covariates were pre-specified while the study was underway and the study data was blinded from the team. Decision
concerning the choice of these covariates as well as the time windows (e.g., 72 hours) were informed by research team consensus. In
particular, these covariates were intended to be proxies for prior engagement. The team selected time windows that were long enough
to capture engagement while short enough to avoid introducing excessive measurement error in the proxy.
Nahum-Shani et al. Page 9
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

(vs. not employing) the reinforcer.
Prior staff contact:
logs of staff emails, messages and
phone calls were used to create a binary indicator for whether (=1) or not (=0) the individual
was contacted prior to randomization. For reciprocity analyses, this indicator was calculated
based on the 24 hours
5
prior to micro-randomization to employing (vs. not employing) the
strategy. For non-monetary reinforcement analyses, this indicator was calculated based on
the 30 hours
5
prior to micro-randomization to employing (vs. not employing) the reinforcer.
Weekend vs. Weekdays:
A binary indicator for whether (=1) or not (=0) the day of the week
is a weekend (Saturday or Sunday).
Analytic Plan for MRT Data
The MRT data was analyzed with a generalization of regression specifically developed to
ensure unbiased estimates of causal effects of time-varying treatments (Boruvka et al., 2018;
Liao et al., 2016). These analyses pool time-varying, longitudinal data across participants.
Here, this regression-based approach is used with a log-link function to accommodate the
binary outcome. The causal effect among available participant days is expressed on the
“risk-ratio” scale, namely on a scale that measures the probability (“risk”) of proximal
self-reporting when an engagement strategy was employed, divided by the probability of
proximal self-reporting when the engagement strategy was not employed. The pre-specified
analytic plan (Rabbi et al., 2017) proposed to consider all participant days as available
for the reciprocity strategy, all participant days in which the daily survey was completed
as available for the entertaining content reinforcer, and all participant days in which the
active tasks were completed as available for the personalized information reinforcer. Here,
availability refers to days in which it is feasible and appropriate to deliver the strategy (see
Boruvka et al., 2018; Klasnja et al., 2015). However, due to unanticipated technical issues
(e.g., software bugs), there were days in which the delivery of the strategies could not occur.
Those participant days were considered unavailable in the current analyses (see Yap et al.,
2020a for details regarding the number of unavailable days for each strategy).
To test the effect of reciprocity, proximal self-reporting refers to the current day; whereas,
to test the effect of non-monetary reinforcement, proximal self-reporting refers to the next
day. Separate analyses were conducted to test the main effects of reciprocity (H1), the
entartaining content reinforcer (H2), and the personalized information reinforcer (H3) on
proximal self-reporting (see Table 1). For reciprocity, the risk-ratio will be greater than 1 if
offering (vs. not offering) a prompt containing an inspirational quote has a causal effect on
the probability of current day self-reporting. For non-monetary reinforcement, the risk-ratio
will be greater than 1 if offering (vs. not offering) the reinforcer after survey completion (for
entartaining content) or active tasks completion (for personalized information) has a causal
effect on the probability of next day self-reporting. Moderators (H4) were tested seperately
for reciprocity and the two non-monetary reinforcers by extending the models used for H1,
H2, and H3 to include covariates intended to investigate moderation of the causal effect of
employing vs. not employing the strategy (Table 2). All analyses controlled for covariates
expected to be highly correlated with self-reporting (i.e., prior day self-reporting, prior app
usage for other reasons, and prior staff contact). These covariates were chosen to reduce the
noise in the effects of engagement strategies (see pre-specified data analytic plan in Open
Science (Rabbi et al., 2017)).
Nahum-Shani et al.
Page 10
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Since some participants were recruited after 4pm and could not be randomized to reciprocity
until the second day of the MRT, we excluded data from the first day of the MRT (i.e.,
29 possible days in analyses). Random assignments were missing for some participants on
available days (i.e., 6, 13 and 22 participants with a total of 108, 21, and 37 days missing
random assignments for reciprocity, entertaining content, and personalized information,
respectively) due to technical issues (e.g., software bugs). All analyses were performed
using complete case data, excluding days with missing random assignments. In sensitivity
analyses, we also report the results based on a summary (Little & Rubin, 1987) of 10
datasets in which the missing value was multiply imputed with one of the two options under
consideration (e.g., reciprocity prompt or no prompt) with 0.5 probability. Details regarding
missing data are provided in Yap et al. (2020a).
Results
Sample Characteristics
Participants were, on average, 20.6 years old (SD = 2.1 years; range 17–24); 54.4% female,
and 70.6% Caucasian. 69.1% had some college and 83.8% had an iPhone. At baseline,
substance use was: 47.1% binge drinking only, 23.5% marijuana use only, and 29.4% both.
Feasibility
Participants completed an average of 60.3% of daily surveys (
M
=18.1,
SD
=9.2), 55.3% of
active tasks (
M
=16.6,
SD
=9.5) and 75.0% of Sunday surveys (
M
=3.0,
SD
=1.2). On average,
participants earned a total of $6.24 (
SD
=$3.83, min=$1.00, max=$13.00) for self-reporting.
Most rated SARA as at least somewhat fun (76.3%) and interesting to use (72.9%). Almost
all participants (96.6%) found the app to be somewhat or very age appropriate. Most liked
or strongly liked the inspirational quotes (62.3%) and the personalized information (66.0%).
However, less than half of participants (46.0%) liked or strongly liked the memes/gifs. In
terms of burden, although nearly all participants perceived SARA as at least somewhat
easy to use (96.6%), 38.0% had periodic or regular technical problems. Most participants
would prefer using SARA to complete surveys, compared to phone-based (79.7%) or text
message-based surveys (71.2%), and most (72.9%) rated SARA as 4.0 stars or higher.
MRT Results
Regarding reciprocity (Table 1), the results indicate that on average individuals are 5%
more likely (Est =
exp
(.05)=1.05; 95% CI: [.97, 1.13]) to self-report on the current day
if an inspirational quote was offered at 4pm versus when not offered. However, there
was insufficient evidence to reject the null hypothesis stating that there is no effect of
this strategy. Regarding non-monetary reinforcement (Table 1), on average, individuals
are 4% less likely (Est=
exp
(.04)=.96; 95% CI: [.88, 1.04]) to self-report on the next
day when entertaining content was offered after survey completion, versus when not
offered. Moreover, on average individuals are 2% less likely (Est =
exp
(−.02)=.98; 95%
CI: [.90, 1.06]) to self-report on the next day when personalized information was offered
after completion of active tasks, versus when not offered. However, there was insufficient
evidence to reject the null hypotheses stating that these non-monetary reinforcers have no
effect on next day self-reporting. In supplementary analyses, we found no evidence of
Nahum-Shani et al.
Page 11
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

sex differences or day-of-study differences in the effects of reciprocity and non-monetary
reinforcement (Yap et al., 2020b)
The moderators’ analysis (Table 2) indicate that the effect of reciprocity varies depending
on whether this strategy was employed during the weekend vs. weekdays (interaction
estimate=.16;
p
<.05), and whether or not the individual used the app for matters unrelated
to self-reporting in the past 72 hours (interaction estimate=−.27;
p
<.10). Employing (vs. not
employing) reciprocity results in only 1% (
exp
(.01)=1.01;
ns
) greater likelihood of current
day self-reporting during week days, yet in 18% (
exp
(.17)=1.18;
p
<.05) greater likelihood
during weekends. Additionally, employing (vs. not employing) this strategy results in only
2% greater likelihood (
exp
(.02)=1.02;
ns
) of current day self-reporting if the individual
used the app for reasons unrelated to self-reporting, yet in 35% (
exp
(.30)=1.35;
p
<.10)
greater likelihood if they did not use the app for reasons unrelated to self-reporting. Effect
moderation was not found statistically significant with respect to the other two candidate
moderators.
Regarding non-monetary reinforcement, the moderators’ analysis indicated that the effect
of offering (vs. not offering) entertaining content immediately after current day survey
completion varies based on prior day self-reporting (interaction estimate=.31;
p
<.05). It is
estimated that offering (vs. not offering) this reinforcer immediately following current day
(
t
) survey completion results in 1% (
exp
(.01)=1.01;
ns
) greater likelihood of next day (
t
+1)
self-reporting if the individual self-reported in the prior day (
t
−1), yet in 25% less likelihood
of next day self-reporting (
exp
(−.29)=.75;
p
<.05) if the individual did not self-report in the
prior day. Effect moderation was not found statistically significant with respect to the other
three candidate moderators.
Lastly, the effect of offering (vs. not offering) personalized information after active tasks
completion varies based on prior day self-reporting (interaction estimate=−.40;
p
<.01)
and prior staff contact (interaction estimate=.20;
p
<.05). Offering (vs. not offering) this
reinforcer after current day (
t
) task completion results in 9% (
exp
(−.10)=.91;
p
<.05) less
likelihood of next day (
t
+1) self-reporting if the individual self-reported in the prior day
(
t
−1), yet 36% (
exp
(.31)=1.36;
p
<.05) greater likelihood if they did not self-report in
the prior day. Next, offering (vs. not offering) this reinforcer after current day (
t
) task
completion results in 9% (
exp
(−.10)=.91;
p
<.05) less likelihood of next day (
t
+1) self-
reporting if the individual did not receive staff contact prior to randomization, yet in 10%
(
exp
(.10)=1.10;
ns
) greater likelihood if they received staff contact prior to randomization.
Effect moderation was not statistically significant with respect to the other two candidate
moderators.
Discussion
This study represents an important step in closing a practical and theoretical gap relating to
the translation of theoretically-grounded engagement strategies into mHealth. Overall, the
results provide initial support for the utility of theoretically-grounded strategies in promoting
mHealth engagement.
Nahum-Shani et al.
Page 12
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Rates of daily self-reporting (e.g., 62.3% overall; 60.3% daily surveys (Mon-Sat); 75%
weekly surveys) were somewhat less than previous ecological momentary assessment
(EMA) studies with substance users, albeit with much lower financial incentives. A meta-
analysis of EMA compliance among substance users of all ages showed that the pooled
estimate was 70.8%; however, studies of A/EAs often find rates of 60–65% (Bonar et al.,
2018; Buckner et al., 2012; Newcomb, Swann, Estabrook, et al., 2018; Newcomb, Swann,
Mohr, et al., 2018; Shorey et al., 2014; Shrier et al., 2018). Our findings are particularly
promising given that the average amount earned (M=$6.24, SD=$3.83, min= $1.00, max=
$13.00) was a fraction of typical compensation provided, potentially reflecting the utility
of the non-monetary engagement strategies in SARA. In addition to improved functionality,
future iterations will attempt to improve non-monetary engagement features in SARA to
reach 80% completion.
Findings from the MRT were supportive of the translation of reciprocity into SARA.
Specifically, individuals were on average 5% more likely to self-report on the current day
when a prompt containing an inspirational quote was offered (vs. not offered) prior to the
start of the self-reporting window. Although this main effect was not statistically significant,
it is higher in magnitude compared to the main effect (3.9% greater likelihood) found in
an MRT study testing the utility of a prompt containing a tailored health message (vs. no
prompt) on proximal engagement in self-reporting (Bidargaddi et al., 2018). Moreover, the
positive effect of reciprocity was amplified under conditions that represent receptivity to
mobile-based prompts (i.e., 18% greater likelihood during the weekend) and vulnerability
to disengagement (i.e., 34% greater likelihood when employed following no app usage
for other reasons). These findings are consistent with acceptability ratings and positive
comments about these messages, with preference for greater personalization.
Concerning the translation of non-monetary reinforcement into SARA, findings from the
MRT were not supportive of using entertaining content to operationalize this strategy.
Individuals were on average 4% less likely (albeit not statistically significant) to self-report
on the next day (
tt
+1) when a non-monetary reinforcer in the form of entertaining content
was offered (vs. not offered) immediately following current day (
tt
) survey completion.
This negative effect was found to be substantially amplified under conditions that represent
vulnerability to disengagement. Specifically, if individuals did not self-report on the
previous day (
tt
−1), offering entertaining content immediately following current day (
tt
)
survey completion resulted in 25% less likelihood of self-reporting on the next day (
tt
+1),
compared to not offering this reinforcer. These findings were consistent with acceptability
ratings, with slightly less than half of participants liking the memes/gifs, and with the mix
of positive and negative comments. In fact, some participants noted that the inspirational
meme/gifs were better than the humorous ones, which were not viewed as particularly funny.
Although we vetted the memes/gifs with similar-aged youth, and despite preliminary testing
indicating that youth liked and perceived the memes/gifs as rewarding (Rabbi et al., 2020),
the results suggest that this type of content may have a short shelf life, may be ineffective
due to the high circulation in daily life, and/or would benefit from greater personalization
due to individual differences.
Nahum-Shani et al.
Page 13
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Findings were more supportive of operationalizing non-monetary reinforcement in the
form of personalized information. On average individuals were 2% less likely (albeit not
statistically significant) to self-report on the next day when this reinforcer was employed
(vs. not employed). However, this effect was positive under conditions that represent
vulnerability to disengagement (i.e., 36% greater likelihood of next day self-reporting,
if no self-reporting on prior day) and receptivity to mobile-based prompts (i.e., 10%
greater likelihood of next day self-reporting under prior staff contact). These findings are
consistent with acceptability ratings and comments suggesting that participants generally
liked the personalized information. However, the effect of this reinforcer was negative under
conditions that represent low vulnerability to disengagement (i.e., 9% less likelihood of
next day self-reporting, if self-reporting on prior day) and less receptivity to mobile-based
prompts (i.e., 9% less likelihood of next day self-reporting, if no prior staff contact). It
is possible that when participants were engaged (i.e., self-reported in the prior day and
did not require staff contact) they were irritated by the use of personalized information
as a reinforcer. This explanation is consistent with acceptability ratings indicating that two-
thirds liked or strongly liked the personalized information, and with comments indicating
they wanted cumulative information available on demand (rather than contingent on self-
reporting), similar to other mobile applications (e.g., steps in Fitbit). Future studies testing
preferences for personalized information could also examine the potential benefits or harms
of summaries regarding improvement vs. a decrement in engagement over time.
Although none of the engagement strategies were found to have a statistically significant
main effect, significant and relatively large effects were found under specific conditions
representing risk for disengagement and receptivity to mobile-based prompts. These findings
may reflect the nature of mHealth intervention prompts, which are delivered in the
individual’s natural environment. In real-life settings, a complex constellation of stable and
dynamic contextual factors may influence the extent that the individual can pay attention to
and act on the prompt (Nahum-Shani et al., 2018). Given that the main effect is an average
effect over time and over any other contextual factors, it is possible that the investigation
of contextual moderators may be more informative in efforts to optimize mobile-based
engagement prompts.
Contrary to expectation, we found no evidence that the effect of reciprocity is moderated
by prior day self-reporting and staff contact, as well as no evidence that the effect
of non-monetary reinforcement is moderated by weekend (vs. weekdays) and prior app
usage for other reasons. While these results may suggest that indicators of vulnerability
and receptivity which are relevant for reciprocity are less relevant for non-monetary
reinforcement and vice versa, a full-scale study is required to validate these results and
draw practical and theoretical conclusions.
Several limitations require acknowledgement. First, minimal financial incentives were
provided in what is fundamentally a non-monetary intervention; this can have implications
on the external validity of the study. Future studies should systematically investigate whether
the results of the current study can be generalized to other settings, including those in which
no financial incentives are provided. Second, future research should investigate whether the
effects of reciprocity and non-monetary reinforcement vary depending on the type of task
Nahum-Shani et al.
Page 14
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

participants are asked to perform (e.g., time to complete, difficulty, frequency and stigma
associated with the behaviors participants are asked to self-report). Third, the utility of non-
monetary reinforcers in SARA may be improved by considering alternative reinforcement
procedures, including starting with a higher rate non-monetary reinforcement schedule and
minimizing the salience of other types of reinforcers such as financial incentives and staff
contact. The optimal reinforcement schedule in this setting should be investigated in future
research. Fourth, the current findings may reflect self-selection bias, as those who enrolled
and remained in the study may be intrinsically motivated, hence view the non-monetary
rewards as less valuable than anticipated. Finally, it is possible that the inspirational
quotes increased engagement by boosting positive affect and cognitive processing, and/or
by serving as a reminder to self-report, as opposed to reciprocity. Future studies should
investigate the mechanisms underlying the effect of such operationalization of reciprocity.
Future studies should also consider developmental differences in adolescents and emerging
adults, as well as seasonal variations in substance use among youth.
Conclusion
Consistent with
Stage I
of the NIH Stage Model (Onken et al., 2014) and the
preparation
phase of MOST (Collins, 2018), this study serves as an early check on the translation of
selected engagement strategies to a particular mHealth setting. Although proof-of-concept
studies are not used to finalize decisions about which component should be included in
optimized interventions, they can be used to pre-screen components if the results indicate
that a certain component is not ready for consideration (Collins, 2018). The results of the
current study provide initial support for the translation of the reciprocity strategy into the
SARA mHealth setting. However, the translation of non-monetary reinforcement requires
further consideration prior to inclusion in a full scale MRT, as it may lead to different
outcomes when operationalized in various ways. These results highlight the importance of
conducting proof-of-concept studies to optimize the translation of engagement strategies into
mHealth settings prior to conducting full scale trials.
Acknowledgement:
This work has been supported by the Michigan Institute for Data Science (PI: Murphy), the University of Michigan
Injury Prevention Center Pilot Study (CDC R49CE002099; PI: Walton), NIH/NIDA P50 DA039838 (PI: Linda
Collins), and NIH/NIDA R01 DA039901; 02R01 DA039901 (PIs: Nahum-Shani; Almirall).
References
Allen TD, Cho E, & Meier LL (2014). Work–family boundary dynamics. Annu. Rev. Organ. Psychol.
Organ. Behav, 1(1), 99–121.
Amico KR (2015). Evidence for technology interventions to promote ART adherence in adult
populations: a review of the literature 2012–2015. Current HIV/AIDS Reports, 12(4), 441–450.
[PubMed: 26412085]
Bidargaddi N, Almirall D, Murphy S, Nahum-Shani I, Kovalcik M, Pituch T, … Strecher V (2018).
To Prompt or Not to Prompt? A Microrandomized Trial of Time-Varying Push Notifications to
Increase Proximal Engagement With a Mobile Health App. JMIR Mhealth Uhealth, 6(11), e10123.
[PubMed: 30497999]
Nahum-Shani et al.
Page 15
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Bonar EE, Cunningham RM, Collins RL, Cranford JA, Chermack ST, Zimmerman MA, … Walton
MA (2018). Feasibility and acceptability of text messaging to assess daily substance use and sexual
behaviors among urban emerging adults. Addict Res Theory 26(2), 103–113. [PubMed: 29632458]
Boruvka A, Almirall D, Witkiewitz K, & Murphy SA (2018). Assessing Time-Varying Causal Effect
Moderation in Mobile Health. Journal of the American Statistical Association, 113(523), 1112–
1121. [PubMed: 30467446]
Brown JD, & Dutton KA (1995). Truth and consequences: The costs and benefits of accurate self-
knowledge. Personality and Social Psychology Bulletin, 21(12), 1288–1296.
Buckner JD, Crosby RD, Silgado J, Wonderlich SA, & Schmidt NB (2012). Immediate antecedents of
marijuana use: An analysis from ecological momentary assessment. Journal of behavior therapy and
experimental psychiatry, 43(1), 647–655. [PubMed: 21946296]
Burger JM, Sanchez J, Imberi JE, & Grande LR (2009). The norm of reciprocity as an internalized
social norm: Returning favors even when no one finds out. Social Influence, 4(1), 11–17.
Butler R, & Nisan M (1986). Effects of no feedback, task-related comments, and grades on intrinsic
motivation and performance. Journal of Educational Psychology, 78(3), 210.
Buu A, Massey LS, Walton MA, Cranford JA, Zimmerman MA, & Cunningham RM (2017).
Assessment methods and schedules for collecting daily process data on substance use related
health behaviors: A randomized control study. Drug alcohol dependence, 178, 159–164. [PubMed:
28651151]
Carver CS, & Scheier MF (1982). Control theory: A useful conceptual framework for personality–
social, clinical, and health psychology. Psychological bulletin, 92(1), 111. [PubMed: 7134324]
Cavanagh K (2010). Turn on, tune in and (don’t) drop out: engagement, adherence, attrition, and
alliance with internet-based interventions. Oxford guide to low intensity CBT interventions, 227–
233.
Cialdini RB (2001). Influence: Science and Practice (4th ed.). Needham Heights, MA: Allyn & Bacon.
Cialdini RB, & Goldstein NJ (2004). Social influence: Compliance and conformity. Annu. Rev.
Psychol, 55, 591–621. [PubMed: 14744228]
Coker KK, Boostrom RE Jr, & Altobello SA (2014). What makes social shoppers click? The role of
social rewards in social shopping. Marketing Management Journal, 24(1), 66–79.
Collins LM (2018). Optimization of Behavioral, Biobehavioral, and Biomedical Interventions: The
Multiphase Optimization Strategy (MOST). Cham, Switzerland: Springer.
De Young R (2000). New ways to promote proenvironmental behavior: Expanding and evaluating
motives for environmentally responsible behavior. Journal of social issues, 56(3), 509–526.
Derricks V, & Earl A (2019). Information Targeting Increases the Weight of Stigma: Leveraging
Relevance Backfires When People Feel Judged. Journal of Experimental Social Psychology, 82,
277–293. doi:10.1016/j.jesp.2018.12.003
Dobson R, Whittaker R, Murphy R, Khanolkar M, Miller S, Naylor J, & Maddison R (2017). The Use
of Mobile Health to Deliver Self-Management Support to Young People With Type 1 Diabetes: A
Cross-Sectional Survey. JMIR Diabetes, 2(1), e4. [PubMed: 30291057]
Dworkin ER, Kaysen D, Bedard-Gilligan M, Rhew IC, & Lee CM (2017). Daily-level associations
between PTSD and cannabis use among young sexual minority women. Addictive behaviors, 74,
118–121. [PubMed: 28618391]
Efklides A (2011). Interactions of metacognition with motivation and affect in self-regulated learning:
The MASRL model. Educational psychologist, 46(1), 6–25.
Fedele DA, Cushing CC, Fritz A, Amaro CM, & Ortega A (2017). Mobile health interventions for
improving health outcomes in youth: a meta-analysis. Jama pediatrics, 171(5), 461–469. [PubMed:
28319239]
Fogg BJ (2002). Persuasive technology: using computers to change what we think and do. Ubiquity,
2002 (December), 2.
Fogg BJ, & Nass C (1997). How users reciprocate to computers: an experiment that demonstrates
behavior change. In CHI’97 extended abstracts on Human factors in computing systems (pp. 331–
332).
Nahum-Shani et al.
Page 16
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Fox RD, & Miner C (1999). Motivation and the facilitation of change, learning, and participation
in educational programs for health professionals. Journal of Continuing Education in the Health
Professions, 19(3), 132–141.
Fredrickson BL (2004). The broaden–and–build theory of positive emotions. Philosophical
Transactions of the Royal Society of London. Series B: Biological Sciences, 359(1449), 1367–
1377. [PubMed: 15347528]
French DP, & Sutton S (2010). Reactivity of measurement in health psychology: how much of a
problem is it? What can be done about it? British journal of health psychology, 15(3), 453–468.
[PubMed: 20205982]
Gouldner AW (1960). The norm of reciprocity: A preliminary statement. American sociological
review, 25(2), 161–178.
Haberer JE, Sabin L, Amico KR, Orrell C, Galárraga O, Tsai AC, … Blaschke TF (2017). Improving
antiretroviral therapy adherence in resource‐limited settings at scale: a discussion of interventions
and recommendations. Journal of the International AIDS Society, 20(1).
Haff N, Patel MS, Lim R, Zhu J, Troxel AB, Asch DA, & Volpp KG (2015). The role of
behavioral economic incentive design and demographic characteristics in financial incentive-based
approaches to changing health behaviors: a meta-analysis. American Journal of Health Promotion,
29(5), 314–323. [PubMed: 25928816]
Hancock DR (2000). Impact of verbal praise on college students’ time spent on homework. The
Journal of Educational Research, 93(6), 384–389.
Heron KE, Lewis RJ, Shappie AT, Dawson CA, Amerson R, Braitman AL, … Kelley ML (2019).
Rationale and Design of a Remote Web-Based Daily Diary Study Examining Sexual Minority
Stress, Relationship Factors, and Alcohol Use in Same-Sex Female Couples Across the United
States: Study Protocol of Project Relate. JMIR Res Protoc, 8(2), e11718. doi:10.2196/11718
[PubMed: 30714946]
Higgins ET, Bond RN, Klein R, & Strauman T (1986). Self-discrepancies and emotional vulnerability:
How magnitude, accessibility, and type of discrepancy influence affect. Journal of personality and
social psychology, 51(1), 5. [PubMed: 3735070]
Hingson RW, Zha W, & White AM (2017). Drinking Beyond the Binge Threshold: Predictors,
Consequences, and Changes in the U.S. Am J Prev Med, 52(6), 717–727. doi:10.1016/
j.amepre.2017.02.014 [PubMed: 28526355]
Hoeppner BB, Stout RL, Jackson KM, & Barnett NP (2010). How good is fine-grained
Timeline Follow-back data? Comparing 30-day TLFB and repeated 7-day TLFB alcohol
consumption reports on the person and daily level. Addict Behav, 35(12), 1138–1143. doi:10.1016/
j.addbeh.2010.08.013 [PubMed: 20822852]
Hull JG, Van Treuren RR, Ashford SJ, Propsom P, & Andrus BW (1988). Self-consciousness and the
processing of self-relevant information. Journal of Personality and Social Psychology, 54(3), 452.
Karekla M, Kasinopoulos O, Neto DD, Ebert DD, Van Daele T, Nordgreen T, … Jensen KL
(2019). Best Practices and Recommendations for Digital Interventions to Improve Engagement
and Adherence in Chronic Illness Sufferers. European Psychologist, 24, 49–67.
Kelly RE, Mansell W, & Wood AM (2015). Goal conflict and well-being: A review and hierarchical
model of goal conflict, ambivalence, self-discrepancy and self-concordance. Personality and
Individual Differences, 85, 212–229.
King G, Currie M, & Petersen P (2014). Child and parent engagement in the mental health intervention
process: a motivational framework. Child and Adolescent Mental Health, 19(1), 2–8. [PubMed:
32878365]
Klasnja P, Hekler EB, Shiffman S, Boruvka A, Almirall D, Tewari A, & Murphy SA
(2015). Microrandomized trials: An experimental design for developing just-in-time adaptive
interventions. Health Psychology, 34(S), 1220–1228.
Kleinginna PR, & Kleinginna AM (1981). A categorized list of motivation definitions, with a
suggestion for a consensual definition. Motivation and emotion, 5(3), 263–291.
Kohler HP, & Thornton R (2012). Conditional Cash Transfers and HIV/AIDS Prevention:
Unconditionally Promising? World Bank Econ Rev, 26(2), 165–190. [PubMed: 24319306]
Nahum-Shani et al.
Page 17
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Lee SA, & Liang Y (2016). The role of reciprocity in verbally persuasive robots. Cyberpsychology,
Behavior, and Social Networking, 19(8), 524–527.
Lent MA (2017). Effects of Text Message Reporting and Reinforcement on Mental Health
Homework Compliance. (Order No. 10250696). Available from ProQuest Dissertations &
Theses Global. (1864629132), Retrieved from http://proxy.lib.umich.edu/login?url=https://search-
proquestcom.proxy.lib.umich.edu/docview/1864629132?accountid=14667
Leonardelli GJ, & Lakin JL (2010). The new adventures of regulatory focus: Self-uncertainty and the
quest for a diagnostic self-evaluation. Handbook of the uncertain self, 216–231.
Liao P, Klasnja P, Tewari A, & Murphy SA (2016). Sample size calculations for micro-randomized
trials in mHealth. Statistics in medicine, 35(12), 1944–1971. [PubMed: 26707831]
Linnemayr S, & Thomas R (2016). Insights from behavioral economics to design more effective
incentives for improving chronic health behaviors, with an application to adherence to
antiretrovirals. Journal of acquired immune deficiency syndromes (1999), 72(2), e50. [PubMed:
26918543]
Little R, JA, & Rubin D,B (1987). Statistical analysis with missing data. Hoboken, NJ: Wiley.
Lizardi D, & Stanley B (2010). Treatment engagement: a neglected aspect in the psychiatric care of
suicidal patients. Psychiatric Services, 61(12), 1183–1191. [PubMed: 21123401]
McPherson SM, Burduli E, Smith CL, Herron J, Oluwoye O, Hirchak K, … Roll JM (2018).
A review of contingency management for the treatment of substance-use disorders: adaptation
for underserved populations, use of experimental technologies, and personalized optimization
strategies. Substance Abuse Rehabilitation 9, 43–57. [PubMed: 30147392]
Michie S, Van Stralen MM, & West R (2011). The behaviour change wheel: a new method for
characterising and designing behaviour change interventions. Implementation science, 6(1), 42.
[PubMed: 21513547]
Michie S, Yardley L, West R, Patrick K, & Greaves F (2017). Developing and evaluating digital
interventions to promote behavior change in health and health care: recommendations resulting
from an international workshop. Journal of medical Internet research, 19(6), e232. [PubMed:
28663162]
Miller WR, & Rollnick S (1991). Motivational Interviewing: Preparing People to Change Addictive
Behavior. New York, NY: Guilford Publications.
Miltenberger RG (2011). Behavior modification: Principles and procedures (5th ed.). Belmont, CA:
Wadsworth Cengage Learning.
Mohr D, Cuijpers P, & Lehman K (2011). Supportive accountability: a model for providing human
support to enhance adherence to eHealth interventions. Journal of medical Internet research, 13(1),
e30. [PubMed: 21393123]
Morrison LG, Hargood C, Pejovic V, Geraghty AW, Lloyd S, Goodman N, … Weal MJ (2017). The
Effect of Timing and Frequency of Push Notifications on Usage of a Smartphone-Based Stress
Management Intervention: An Exploratory Trial. PloS one, 12(1), e0169162. [PubMed: 28046034]
Nahum-Shani I, Hekler E, & Spruijt-Metz D (2015). Building health behavior models to guide the
development of just-in-time adaptive interventions: a pragmatic framework. Health Psychology
34(Supp), 1209–1219.
Nahum-Shani I, Smith SN, Spring BJ, Collins LM, Witkiewitz K, Tewari A, & Murphy SA (2018).
Just-in-Time Adaptive Interventions (JITAIs) in Mobile Health: Key Components and Design
Principles for Ongoing Health Behavior Support. Annals of Behavioral Medicine, 52, 446–462.
doi:10.1007/s12160-016-9830-8 [PubMed: 27663578]
Newcomb ME, Swann G, Estabrook R, Corden M, Begale M, Ashbeck A, … Mustanski B (2018).
Patterns and predictors of compliance in a prospective diary study of substance use and sexual
behavior in a sample of young men who have sex with men. Assessment, 25(4), 403–414.
[PubMed: 27586686]
Newcomb ME, Swann G, Mohr D, & Mustanski B (2018). Do diary studies cause behavior change?
An examination of reactivity in sexual risk and substance use in young men who have sex with
men. AIDS and Behavior, 22(7), 2284–2295. [PubMed: 29332235]
Onken LS, Carroll KM, Shoham V, Cuthbert BN, & Riddle M (2014). Reenvisioning Clinical Science:
Unifying the Discipline to Improve the Public Health. Clinical psychological science : a journal
Nahum-Shani et al.
Page 18
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

of the Association for Psychological Science, 2(1), 22–34. doi:10.1177/2167702613497932
[PubMed: 25821658]
Parsons K, Butavicius M, Delfabbro P, & Lillie M (2019). Predicting susceptibility to social influence
in phishing emails. International Journal of Human-Computer Studies, 128, 17–26. doi:10.1016/
j.ijhcs.2019.02.007
Patrick ME, Terry-McElrath YM, Schulenberg JE, & Bray BC (2017). Patterns of high-intensity
drinking among young adults in the United States: A repeated measures latent class analysis.
Addict Behav, 74, 134–139. doi:10.1016/j.addbeh.2017.06.004 [PubMed: 28628871]
Pekrun R (2006). The control-value theory of achievement emotions: Assumptions, corollaries, and
implications for educational research and practice. Educational psychology review, 18(4), 315–
341.
Pellowski JA, & Kalichman SC (2012). Recent advances (2011–2012) in technologydelivered
interventions for people living with HIV. Current HIV/AIDS Reports, 9(4), 326334.
Perski O, Blandford A, West R, & Michie S (2016). Conceptualising engagement with digital
behaviour change interventions: a systematic review using principles from critical interpretive
synthesis. Translational behavioral medicine, 7(2), 254–267.
Perugini M, Gallucci M, Presaghi F, & Ercolani AP (2003). The personal norm of reciprocity.
European Journal of Personality, 17(4), 251–283.
Rabbi M, Kotov MP, Cunningham R, Bonar EE, Nahum-Shani I, Klasnja P, … Murphy S (2018).
Toward increasing engagement in substance use data collection: development of the Substance
Abuse Research Assistant app and protocol for a micro-randomized trial using adolescents and
emerging adults. JMIR Research Protocols, 7(7), e166. [PubMed: 30021714]
Rabbi M, Philyaw-Kotov M, Klasnja P, Bonar E, Nahum-Shani I, Walton M, & Murphy S (2017).
SARA – 005substance Abuse Research Assistant. Retrieved from 10.17605/OSF.IO/VWZMD
Rabbi M, Philyaw-Kotov M, Li J, Li K, Rothman B, Giragosian L, Reyes M, Gadway H, Cunningham
R, Bonar E, Nahum-Shani I, Walton M, Murphy SA, & Klasnja P (2020). Translating Behavioral
Theory into Technological Interventions: Case Study of an mHealth App to Increase Self-reporting
of Substance-Use Related Data. arXiv preprint arXiv:2003.13545.
Raes A, Schellens T, De Wever B, & Vanderhoven E (2012). Scaffolding information problem solving
in web-based collaborative inquiry learning. Computers & Education, 59(1), 82–94. doi:10.1016/
j.compedu.2011.11.010
Research Kit. (2018). Active tasks in Apple Research Kit. Retrieved from http://researchkit.org/docs/
docs/ActiveTasks/ActiveTasks.html
Rivis A, Abraham C, & Snook S (2011). Understanding young and older male drivers’ willingness
to drive while intoxicated: The predictive utility of constructs specified by the theory of planned
behaviour and the prototype willingness model. British journal of health psychology, 16(2), 445–
456. [PubMed: 21489069]
Robbins R, Krebs P, Jagannathan R, Jean-Louis G, & Duncan TD (2017). Health App Use Among
US Mobile Phone Users: Analysis of Trends by Chronic Disease Status. JMIR Mhealth Uhealth,
5(12), e197. doi:10.2196/mhealth.7832 [PubMed: 29258981]
Roberts AL, Fisher A, Smith L, Heinrich M, & Potts HW (2017). Digital health behaviour change
interventions targeting physical activity and diet in cancer survivors: a systematic review and
meta-analysis. Journal of Cancer Survivorship, 11(6), 704–719. [PubMed: 28779220]
Saberi P, & Johnson MO (2015). Correlation of internet use for health care engagement purposes
and HIV clinical outcomes among HIV-positive individuals using online social media. Journal of
health communication, 20(9), 1026–1032. [PubMed: 26120890]
Shaw SD, Yoon C, Wagner B, & Nahum-Shani I (2019). Engagement in a digital world: An organizing
framework for engagement strategies. Paper presented at the Society for Consumer Psychology
Annual Conference, Savannah, GA.
Shelton JL, & Levy RL (1981). Behavioral assignments and treatment compliance: A handbook of
clinical strategies. Champaign, IL: Research Press.
Shorey RC, Stuart GL, Moore TM, & McNulty JK (2014). The temporal relationship between alcohol,
marijuana, angry affect, and dating violence perpetration: A daily diary study with female college
students. Psychology of Addictive Behaviors, 28(2), 516. [PubMed: 24274434]
Nahum-Shani et al.
Page 19
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Shrier LA, Burke PJ, Kells M, Scherer EA, Sarda V, Jonestrask C, … Harris SK (2018). Pilot
randomized trial of MOMENT, a motivational counseling-plus-ecological momentary intervention
to reduce marijuana use in youth. Mhealth, 4(29).
Simblett S, Greer B, Matcham F, Curtis H, Polhemus A, Ferrão J, … Wykes T (2018). Barriers to and
facilitators of engagement with remote measurement technology for managing health: systematic
review and content analysis of findings. Journal of medical Internet research, 20(7), e10480.
[PubMed: 30001997]
Singh K, Drouin K, Newmark LP, Rozenblum R, Lee J, Landman A, … Bates DW (2016).
Developing a framework for evaluating the patient engagement, quality, and safety of mobile
health applications. Issue Brief (Commonw Fund), 5(1), 11.
Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, & Mani M (2015). Mobile app
rating scale: a new tool for assessing the quality of health mobile apps. JMIR mHealth and
uHealth, 3(1), e27. [PubMed: 25760773]
Strang S, Park S, Strombach T, & Kenning P (2016). Applied economics: The use of monetary
incentives to modulate behavior. In Progress in brain research (Vol. 229, pp. 285301). Amsterdam,
The Netherlands Elsevier.
Swendeman D, Ramanathan N, Baetscher L, Medich M, Scheffler A, Comulada WS, & Estrin D
(2015). Smartphone self-monitoring to support self-management among people living with HIV:
Perceived benefits and theory of change from a mixed-methods, randomized pilot study. Journal of
acquired immune deficiency syndromes 69, S80–91. [PubMed: 25867783]
Taylor S, Ferguson C, Peng F, Schoeneich M, & Picard RW (2019). Use of In-Game Rewards to
Motivate Daily Self-Report Compliance: Randomized Controlled Trial. Journal of medical Internet
research, 21(1), e11683. [PubMed: 30609986]
Van den Bos K (2009). Making sense of life: The existential self trying to deal with personal
uncertainty. Psychological Inquiry, 20(4), 197–217.
Wray TB, Merrill JE, & Monti PM (2014). Using ecological momentary assessment (EMA) to assess
situation-level predictors of alcohol use and alcohol-related consequences. Alcohol research:
current reviews, 36(1), 19–27. [PubMed: 26258997]
Yap J, Rabbi M, Philyaw-Kotov M, Walton M, Murphy S, & Nahum-Shani I (2020a). SARA:
Availability and Missing Data Summaries. Retrieved from https://github.com/jamieyap/SARA/
blob/master/sara-tables-main.pdf
Yap J, Rabbi M, Philyaw-Kotov M, Walton M, Murphy S, & Nahum-Shani I (2020b). SARA: Results.
Retrieved from https://github.com/jamieyap/SARA/blob/master/displayresults.pdf
Nahum-Shani et al. Page 20
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Figure 1.
The Need, Ability & Motivation (NAM) logic model
Nahum-Shani et al. Page 21
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
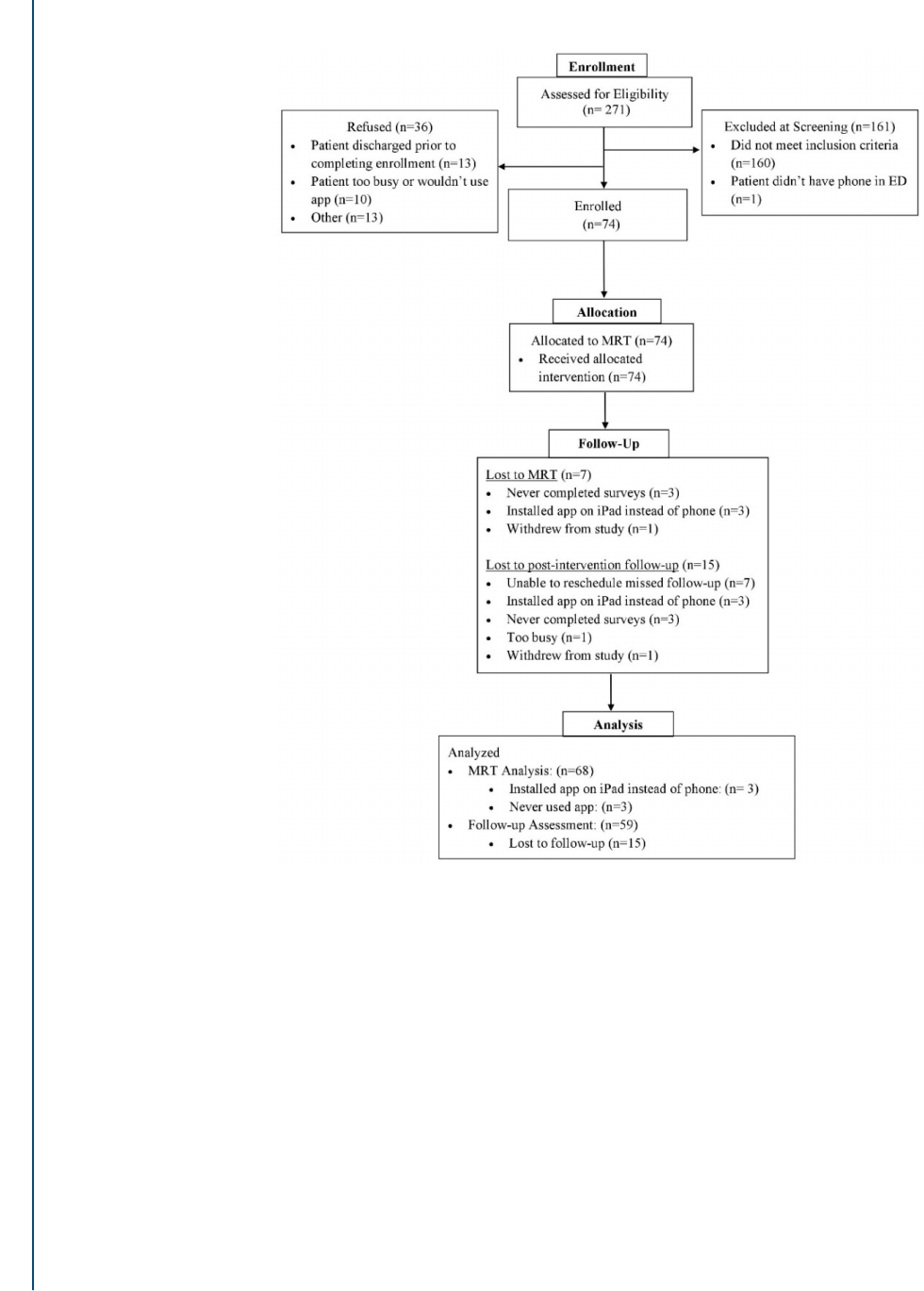
Figure 2.
MRT Consort Diagram for Study Enrollment
Nahum-Shani et al. Page 22
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript

Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Nahum-Shani et al. Page 23
Table 1:
Main Effect Analyses
Main effect analyses
1
Reciprocity Strategy (N= 68) Non-Monetary Reinforcer
Entertaining Content (N= 50) Personalized Information (N=50)
Beta
(Imputed
2
)
SE
(Imputed
2
)
Exp (beta)
(Imputed
2
)
Beta
(Imputed
2
)
SE
(Imputed
2
)
Exp (beta)
(Imputed
2
)
Beta
(Imputed
2
)
SE
(Imputed
2
)
Exp (beta)
(Imputed
2
)
Causal effect
3
(engagement
strategy=yes)
.05
(.05)
.04
(.04)
1.05 [.97, 1.13]
(1.05) [.97,
1.13]
−.04
(−.04)
.04
(.03)
.96 [.88, 1.04]
(.97) [.91, 1.03]
−.02
(−.02)
.04
(.04)
.98 [.90, 1.06]
(.98) [.90, 1.06]
Control
Variables
4
App usage
outside of
self-reporting
(yes=1)
.63
**
(.48
**
)
.17
(.18)
1.89 [1.26, 2.52]
(1.61) [1.04,
2.18]
.13
(.10)
.10
(.08)
1.13 [.91, 1.35]
(1.11) [.94,
1.28]
.01
(−.01)
.08
(.06)
1.01 [.85, 1.17]
(1.00) [.88,
1.12]
Prior day
self-reporting
(yes=1)
.42
**
(.49
**
)
.11
(.13)
1.52 [1.19, 1.85]
(1.64) [1.22,
2.06]
.25
**
(.24
**
)
.07
(.07)
1.28 [1.10, 1.46]
(1.27) [1.10,
1.44]
.22
**
(.24
**
)
.08
(.07)
1.25 [1.05, 1.45]
(1.28) [1.10,
1.46]
Prior contact
by study staff
(yes=1)
−.17
**
(−.18
**
)
.04
(.04)
.84 [.77, .91]
(.83) [.76, .90]
−.08
†
(−.07
†
)
.04
(.04)
.92 [.85, .99]
(.93) [.86, 1.00]
−.09
†
(−.09
†
)
.05
(.05)
.91 [.82, 1.00]
(.91) [.82, 1.00]
†
p
<0.10
*
p
<0.05
**
p
<0.01
95% Confidence Intervals are provided in the square brackets— [lower bound, upper bound].
1.
Both hypotheses as well as control variables are pre-specified (see open science protocol in Rabbi et al., 2017).
2.
Imputed =summary based on 10 imputed datasets
3.
For reciprocity strategy, the term ‘effect’ refers to 4pm prompt relative to no 4pm prompt; for the non-monetary reinforcers ‘effect’ refers to offering a reinforcer relative to no reinforcer following survey
(for entertaining content) or active tasks (for personalized information) completion.
4.
Although estimates pertaining to the control variables are provided for completeness, we caution readers against interpreting them since correct specification of this part of the model is not required to
yield consistent estimates of the causal effect of the randomized engagement strategies (see Boruvka et al., 2016).
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Nahum-Shani et al. Page 24
Table 2:
Summary of Moderation Analyses
Moderation Analyses
3
Reciprocity Strategy (N= 68 participants, D=
1954 days)
Non-Monetary Reinforcer
Entertaining Content (N= 50 participants, D=
1400 days)
Personalized Information (N= 50 participants,
D= 1300 days)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Moderator:
Weekend (=1)
vs. weekdays
(=0)
Effect
2
on
week days
.01
(.00)
.05
(.05)
1.01
(1.00)
−.03
(−.03)
.05
(.05)
0.97
(.97)
.01
(.01)
.05
(.05)
1.01
(1.01)
Effect
2
on
weekend days
.17
*
(.16
*
)
.07
(.07)
1.18
(1.18)
−.04
(−.04)
.06
(.07)
.96
(.96)
−.12
(−.12)
.08
(.08)
.89
(.89)
Interaction
.16
*
(.16
*
)
.08
(.08)
1.17
(1.17)
−.01
(−.01)
.09
(.09)
.99
(.99)
−.13
(−.12)
.10
(.10)
.88
(.89)
Moderator: Prior
contact by study
staff (yes=1;
no=0)
Effect
2
when
prior contact
=no
.02
(.02)
.05
(.05)
1.02
(1.02)
−.03
(−.03)
.05
(.05)
.97
(.97)
−.10
*
(−.09
†
)
.05
(.05)
.91
(.92)
Effect
2
when
prior
contact=yes
.10
(.10)
.07
(.07)
1.11
(1.10)
−.05
(−.04)
.06
(.06)
.95
(.96)
.10
(.10)
.08
(.08)
1.10
(1.10)
Interaction .08
(.08)
.07
(.08)
1.09
(1.08)
−.02
(−.02)
.08
(.08)
.98
(.99)
.20
*
(.19
*
)
.09
(.09)
1.22
(1.20)
Moderator: Prior
app usage for
other reasons
(yes=1; no=0)
Effect
2
when
app usage =no
.30
†
(.19)
.16
(.16)
1.35
(1.21)
−.06
(−.06)
.14
(.13)
.94
(.94)
−.14
(−.09)
.13
(.11)
.87
(.92)
Effect
2
when
app usage =yes
.02
(.02)
.04
(.04)
1.02
(1.02)
−.03
(−.03)
.04
(.04)
.97
(.97)
−.02
(−.02)
.04
(.04)
.98
(.98)
Interaction
−.27
†
(−.17)
.16
(.16)
.76
(.85)
.03
(.03)
.15
(.14)
1.03
(1.03)
.12
(.07)
.14
(.12)
1.13
(1.07)
Moderator: Prior
day self-
reporting (yes=1;
no=0)
Effect
2
when
prior day self-
report =no
.15
(.13)
.11
(.12)
1.16
(1.13)
−.29
*
(−.28
*
)
.13
(.13)
.75
(.76)
.31
*
(.28
*
)
.13
(.13)
1.36
(1.32)
Effect
2
when
prior day self-
report =yes
.03
(.02)
.04
(.04)
1.03
(1.03)
.01
(.01)
.04
(.04)
1.01
(1.01)
−.10
*
(−.09
†
)
.05
(.04)
.91
(.92)
Health Psychol
. Author manuscript; available in PMC 2022 January 07.

Author Manuscript Author Manuscript Author Manuscript Author Manuscript
Nahum-Shani et al. Page 25
Moderation Analyses
3
Reciprocity Strategy (N= 68 participants, D=
1954 days)
Non-Monetary Reinforcer
Entertaining Content (N= 50 participants, D=
1400 days)
Personalized Information (N= 50 participants,
D= 1300 days)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Beta
(Imputed
1
)
SE
(Imputed
1
)
Exp (beta)
(Imputed
1
)
Interaction −.12
(−.10)
.11
(.11)
.89
(.91)
.31
*
(.29
*
)
.13
(.13)
1.36
(1.34)
−.40
**
(−.36
**
)
.14
(.13)
.67
(.67)
†
p
<0.10
*
p
<0.05
**
p
<0.01
1.
Imputed =summary based on 10 imputed datasets
2.
For reciprocity strategy, the term ‘effect’ refers to 4pm prompt relative to no 4pm prompt; for the non-monetary reinforcers ‘effect’ refers to offering a reinforcer relative to no reinforcer following survey
(for entertaining content) or active tasks (for personalized information) completion.
3.
Moderation analyses include the same control covariates as in main effect analysis; for brevity we did not include information concerning their estimated parameters in the table.
Health Psychol
. Author manuscript; available in PMC 2022 January 07.
